

Translate this page into:
Gastric MALT-lymphoma with Mott cell differentiation
Address for correspondence: Dr. Nalini GuptaC6/18, Second Floor, Ardee City, Sector 52, Gurgaon, Haryana, India. drnalinibansal@yahoo.com
This article was originally published by Thieme Medical and Scientific Publishers Private Ltd. and was migrated to Scientific Scholar after the change of Publisher.
We report a case of an 80-year-old male presented with complaints of early satiety and difficulty in eating for past 1 year. Gastroduodenoscopy done showed small hiatus hernia in esophagus with edematous mucosa and venous blebs. Large ulceroproliferative growth was noted in cardia and fundus. The body of stomach showed large superficial spreading ulceration with elevated edges along the lesser sac. Antrum and pylorus appear unremarkable. A biopsy was taken from the growth and send for histopathological examination. Biopsy tissue from the mass showed variable distortion of foveolar architecture. Lamina propria shows diffuse infiltrate of Mott cells with multiple cytoplasmic eosinophilic inclusions along with dense diffuse infiltrate of lymphoid cells. Giemsa stain done for Helicobacter pylori was negative. These plasma cells with Mott cell differentiation are seen infiltrating the superficial lamina propria and seen amidst gastric glands and focally destroying them forming lymphoepithelial lesions Figure 1. Immunohistochemistry performed showed positive staining for leukocyte common antigen, CD 20 and negative staining for Pan-cytokeratin.
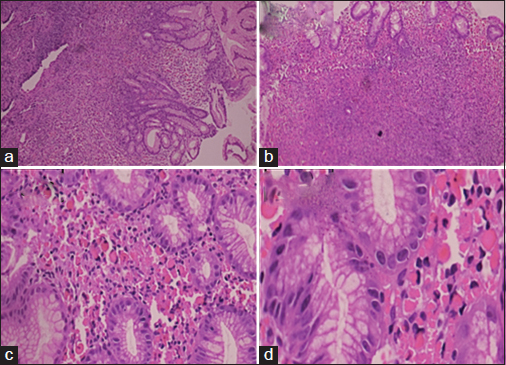
- (a) Diffuse sheets of lymphocytes in lamina propria (H and E, ×10). (b) Diffuse sheets of lymphocytes admixed with plasma cells (H and E, ×10). (c) Numerous Mott cells in superficial lamina (H and E, ×40). (d) Numerous Mott cells with itracytoplasmic eosinophilic inclusion (H and E, ×100)
The patient refused to receive chemotherapy for the same, so treatment via radiotherapy was planned. External beam radiotherapy by 6 MV photons from linear accelerator was started. He received 36Gy in 20 fractions by IMRT in total 20 sittings over a period of 1 month Figure 2. After completion of radiotherapy, a repeat endoscopic examination was performed which revealed completely healed lesion in fundus and body of the stomach. Gastric MALT-lymphoma with prominent Mott cell differentiation is very rare with very few cases reported in literature until date.1,2,3 There is no consensus on to treatment guidelines for these patients, and our case might add to radiotherapy being considered as a primary treatment modality in these patients especially those who are H. pylori negative. The differential diagnosis of Russell body gastritis also needs to be excluded in these cases and finding of a mass on endoscopy and lymphoepithelial lesions on histology are a useful guide to a malignant pathology.
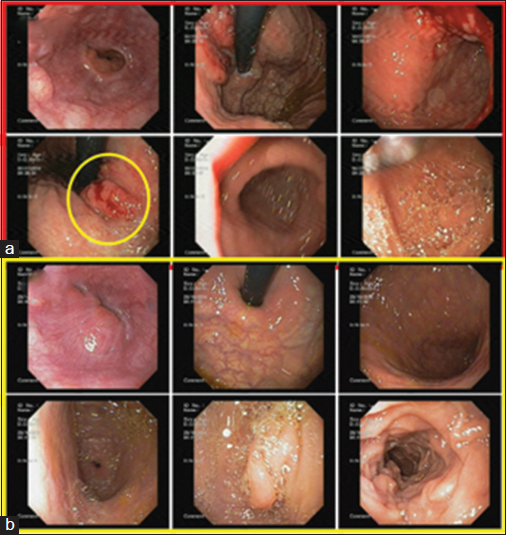
- (a) Upper gastrointestinal endoscopy showing mass in fundus and cardia. (b) Follow-up upper gastrointestinal endoscopy showing no residual mass
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Stomach MALT-lymphoma with marked plasmocytic differentiation: A variant of Mott's cell tumor. Arkh Patol. 2004;66:40-2.
- [Google Scholar]
- Malignant plasmatic gastric lymphoma secreting IgA-kappa. Case report with histo-immunofluorescent study (author's transl)Arch Anat Cytol Pathol. 1979;27:209-12.
- [Google Scholar]
- A case of mucosa-associated lymphoid tissue lymphoma of the gastrointestinal tract showing extensive plasma cell differentiation with prominent Russell bodies. World J Clin Cases. 2013;1:176-80.
- [Google Scholar]




