

Translate this page into:
A Case of Plasma Cell Myeloma with Multilobated and Monocytoid Morphology
Address for correspondence Jyoti Sawhney, MD, DM, Department of Oncopathology, The Gujarat Cancer & Research Institute, Ahmedabad, Gujarat, 380016, India. jyoti.sawhney@gcriindia.org
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Plasma cell myeloma (PCM) accounts for approximately 1% of malignant tumors and 10 to 15% of hematological neoplasms. It is a malignant disease characterized by abnormal proliferation of plasma cells and monoclonal immunoglobulins or free light chains (FLCs). There are many morphological variations of the myeloma plasma cells which include mature, immature, plasmablastic, and pleomorphic types. Here, we report a rare presentation of PCM with normal serum protein electrophoresis but elevated serum FLCs and having convoluted, multilobated, and monocytoid morphology. This type of morphology is related to an aggressive clinical course and resistance to conventional chemotherapy. Moreover, absence of M protein in serum/urine electrophoresis does not rule out the diagnosis of PCM and serum FLC assays plays an important role in this kind of scenarios.
Keywords
light chain myeloma
monocytoid
multilobated

Introduction
Plasma cell myeloma (PCM) accounts for approximately 1% of malignant tumors and 10 to 15% of hematological neoplasms.1 Bone marrow studies are performed for confirmation of diagnosis, even when the clinical, laboratory, and radiological findings are evident. There are many morphological variations of the myeloma plasma cells which include mature, immature, plasmablastic, and pleomorphic types. Approximately 2% of myelomas are distinguished by marked nuclear lobation and convolutions.2 We report a case of PCM, that presented with convoluted, multilobated, and monocytoid nuclei, without detectable myeloma protein in the serum or urine and had a very aggressive clinical course.
Case Presentation
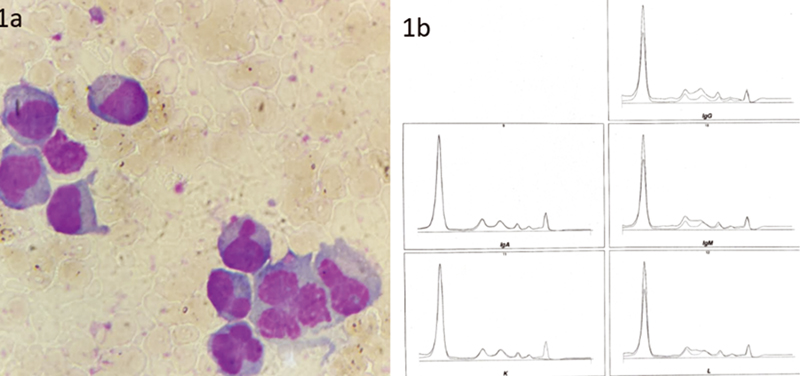
A 43-year-old lady presented with back pain and generalized weakness. Physical examination revealed pallor. Laboratory results are shown in Table 1. X-ray pelvis with both hips showed few well-defined lytic lesions with nonsclerotic margins in bilateral innominate bones and upper end of both femurs. Bone marrow aspiration was done and it showed increased plasma cells (20%) showing mature and immature plasma cells with convolution and multilobation (Fig. 1A). Bone marrow biopsy also showed features of PCM. Following which the myeloma workup was done and results are shown in Table 1. No M band was detected on serum protein electrophoresis. Serum immunofixation showed only kappa light chain (Fig. 1B). Free light chain assay showed increased free kappa light chain and free kappa-to-lambda chain ratio. Hence, a diagnosis of light chain multiple myeloma (LCMM) was made and the patient received combined chemotherapy of bortezomib, lenalidomide, and dexamethasone. After completion of chemotherapy at the end of 4 months, laboratory tests and other relevant investigations were repeated and the findings are shown in Table 1. Bone marrow aspiration and biopsy showed 90% plasma cells with marked pleomorphism showing convoluted and multilobulated morphology and diffuse sheets of highly pleomorphic plasma cells, respectively. She was given the option for bone marrow transplantation but due to monetary issues she opted for combined chemotherapy (pomalidomide, carfilzomib, and dexamethasone). She was followed up to 7 months and was alive till last follow-up.
-
Fig. 1 (A) Bone marrow aspirate showing convoluted, multilobulated, and monocytoid plasma cells. May-Grunwald-Giemsa stain (MGG) ×100. (B) Serum immunofixation showing kappa light chain only.
|
First visit |
After 4 months |
|
|---|---|---|
|
HB |
9.4 g/dL |
7 g/dL |
|
WBC |
5.2 × 10^3/µL |
4.59 × 10^3/µL |
|
Platelet |
30 × 10^3/µL |
14 × 10^3/µL |
|
Serum calcium |
7.89 mg/dL |
6.8 mg/dL |
|
Serum creatinine |
0.77 mg/dL |
0.7 mg/dL |
|
Beta-2 microglobulin |
4.32 mg/dL |
3.49 mg/L |
|
Serum total protein |
5.52 g/dL |
5.49 g/dL |
|
Serum albumin |
3.10 g/dL |
2.4 g/dL |
|
Serum globulin |
2.42 g/dL |
3.09 g/dL |
|
Alpha 1 globulin |
0.43 g/dL |
0.7 g/dL |
|
Alpha 2 globulin |
1.04 g/dL |
1.6 g/dL |
|
Beta 1 globulin |
0.49 g/dL |
0.4 g/dL |
|
Beta 2 globulin |
0.21 g/dL |
0.2 g/dL |
|
Gamma globulin |
0.25 g/dL |
0.2 g/dL |
|
Albumin:Globulin ratio |
1.28 |
0.76 |
|
M band on serum electrophoresis |
Not detected. |
Not detected |
|
Serum immunofixation |
Kappa chain detected |
Kappa chain detected |
|
Serum IgA level, by nephelometry |
32 mg/dL |
43 mg/dL |
|
Serum IgG level, by nephelometry |
300 mg/dL |
597 mg/dL |
|
Serum IgM level, by nephelometry |
7 mg/dL |
15 mg/dL |
|
Free kappa (light chain) |
144 mg/dL |
196 mg/dL |
|
Free lambda (light chain) |
1.5 mg/dL |
44 mg/dL |
|
Free kappa/lambda light chain ratio |
96 |
4.45 |
Abbreviations: HB, hemoglobin; Ig, immunoglobulin; WBC, white blood cell.
Discussion
PCM is a bone marrow-based, multifocal plasma cell neoplasm associated with a M protein in serum or urine.3 Various morphological subtypes are present. In the current case, bone marrow showed cleaved and multilobulated plasma cells; however, the lady did not show any M protein on immunoelectrophoresis. Nonsecretory myeloma is a rare subgroup of PCM which accounts for 3% of all PCM.3 In these cases, the plasma cells fail to secrete immunoglobulin and no serum/urine M protein was found. In two-thirds of these cases, elevated serum free light chains or an abnormal free light chain ratio is observed.4 Serum free light chain assays in our case revealed elevated free light chains and she was diagnosed with LCMM. LCMM is the third most common type of PCM and carries a grim prognosis.5 Moreover, plasma cells from PCM patients showing irregular nuclei indicate more advanced stage of the disease and worse prognosis.6 PCM with multinucleated plasma cells is a rare morphological variant, which usually presents with light chain expression and is characterized by an aggressive course and resistance to conventional chemotherapy.7 The lady in our case had relapsed myeloma activity after six cycles of combined bortezomib-based chemotherapy. Patients with active myeloma are often given a combination of two or three drugs. Often, a combined drug therapy containing bortezomib, lenalidomide, and dexamethasone is used. There are also many regimes for previously treated PCM according to the National Comprehensive Cancer Network guidelines, version 7, 2021. Molecular diagnostics play an important role to predict the prognosis. The negative prognostic impact of specific immunoglobulin heavy chain (IgH) translocations such as t(4;14), t(14;16), chromosome 13 deletion by conventional cytogenetics, and loss of 17p13 by interphase fluorescence in situ hybridization are now established.8
Conclusion
This case was presented due to its unique morphology which was found in the context of LCMM. Further genetic studies are required to show the association of IgH or p53 mutation with this sort of morphology, aggressive clinical course, and resistance to conventional chemotherapy.
Conflict of Interest
None declared.
References
- Clinico-hematological profile of multiple myeloma in a teaching hospital - a 2 year study. IP Arch Cytol Histopathol Res. 2019;4(04):305-309.
- [Google Scholar]
- Neoplasia In: Kaplan L A, Pesce A J, eds. Clinical Chemistry: Theory, Analysis, Correlation (5th ed.). Missouri: Mosby Elsevier; 2010. p. :1051-1067.
- [Google Scholar]
- WHO Classification of Tumours of Haematopoetic and Lymphoid Tissues In: Revised (4th ed.). Lyon, France: IARC Press; 2017.
- [Google Scholar]
- Serum free light-chain measurements for identifying and monitoring patients with nonsecretory multiple myeloma. Blood. 2001;97(09):2900-2902.
- [Google Scholar]
- Light chain multiple myeloma, clinic features, responses to therapy and survival in a long-term study. World J Surg Oncol. 2014;12:234.
- [Google Scholar]
- Myeloma cell morphology and morphometry in correlation with clinical stages and survival. Diagn Cytopathol. 2013;41(11):947-954.
- [Google Scholar]
- Multiple myeloma with multilobated plasma cell nuclei. Turk J Haematol. 2011;28(02):158-159.
- [Google Scholar]
- Prognostic and therapeutic significance of myeloma genetics and gene expression profiling. J Clin Oncol. 2005;23(26):6339-6344.
- [Google Scholar]




