

Translate this page into:
Serrated adenoma of stomach: A premalignancy?
Address for correspondence: Dr. Divya A, Department of Pathology, Meenakshi Medical College and Research Institute, Kanchipuram, Tamil Nadu - 631 552, India. diya_ail@yahoo.com
This article was originally published by Thieme Medical and Scientific Publishers Private Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Serrated adenoma is a newly described entity in the group of gastric adenomas. Until date only 20 cases of gastric serrated adenoma have been reported. It is an important entity to be diagnosed accurately as it has a very high-risk of malignant transformation, especially those located in the cardia of stomach. Serrated adenoma associated with adenocarcinoma is more frequent in the elderly, but pure serrated adenoma is common in the young, in whom follow-up is mandatory. Gastric serrated adenoma has distinct location, definite histomorphology and characteristic Ki-67 immunohistochemical staining. Ki-67 staining helps to differentiated pure serrated adenoma from those associated with adenocarcinoma. We present a young adult male, incidentally detected to have gastric serrated adenoma.
Keywords
Ki-67
premalignancy
serrated adenoma
stomach

Introduction
Adenomas of the stomach, according to WHO are classically divided into villous, tubular, and mixed type.1 Serrated adenoma is a novel entity added to this group recently. Serrated adenoma through a common terminology in the colon is a very rare pathology in the stomach. The first case of gastric serrated adenoma was reported in the year 2001 by Rubio,2 after which literature search revealed only 20 reported cases till date.3 Serrated adenoma is a polypoidal growth composed of glands showing lateral saw tooth-like notches produced by the scalloped epithelial indentation which exhibit dysplastic changes.2 It is an important entity to be diagnosed early and accurately, as it has increased the risk of progression to invasive carcinoma. The literature search reveals (75%) 15 of the 20 reported cases to have an associated invasive component or progress to carcinoma on follow-up.3 We report one such rare case of serrate adenoma in the antrum of the stomach in a 27-year-old male patient, detected incidentally on a routine gastroscopy.
Case Report
A 27-year-old male patient presented with epigastric pain and burning sensation. He is an alcoholic and smokes occasionally. His past or family history was not contributory. A provisional diagnosis of gastroesophageal reflux disease was made and followed by gastroscopy to rule out gastric ulcer or gastric neoplasm. Gastroscopy reveled a polypoidal lesion in the antrum of the stomach which was biopsied.
On gross examination, multiple, tiny grey white soft tissue bits were seen. On microscopy, polypoidal growth, lined by epithelial cells showing scalloping of the margins was noted. These epithelial cells showed multilayering at places and atypia with enlargement of the nuclei. No areas of invasion of these atypical cells or glands were shown in Figure 1. The slides were then submitted for the immunohistochemical (IHC) study for Ki-67, which showed classical staining pattern of serrated adenoma showing intermittent positivity of submucosal glands and lining epithelium of the polyp Figure 2. Diagnosis of serrated adenoma of the antrum of the stomach was made.
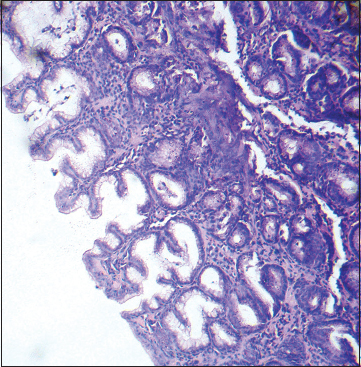
- Gastric serrated adenoma showing serrated epithelium with scalloped margins with subepithelial glands showing focal hyperchromasia (H and E, staining ×400)
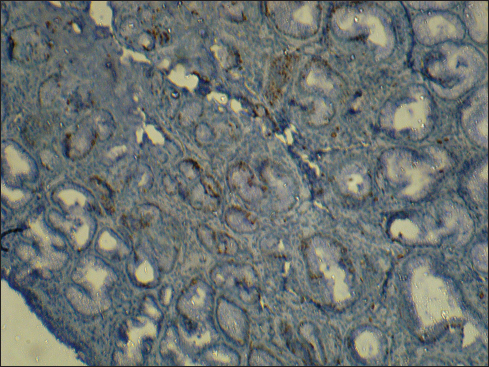
- Ki-67 immunohistochemistry showing positivity of subepithelial glands and intermittent positivity of serrated epithelium (Ki-67 ×100)
Discussion
Gastric polyps are identified incidentally during 2–6% of upper gastrointestinal endoscopies.4 These polyps are traditionally classified into hyperplastic polyps and adenomas.4 Serrated adenoma is a recently described rare entity amongst the gastric adenoma group, with an incidence of 20 reported cases and majority (75%) having an associated malignancy.3 Serrated adenoma of the stomach occurs sporadically, but its occurrence in patients with hereditary trait has also been known. Rubio and Björk reported a case of gastric serrated adenoma with invasive carcinoma in a patient of Lynch syndrome.3
Though serrated adenoma of the stomach has been mistaken as villous adenoma in the past due to similar appearances, it has distinct localization and definite morphological features and higher risk of transformation to carcinoma in comparison to villous adenoma.1,5
Serrated adenoma has also been reported in an appendix, duodenum, pancreatic duct, and Barrett's esophagus and is followed up for an associated malignancy.3
An interesting observation revealed during literature search was the occurrence of serrated adenoma of the stomach in two extremes of age groups. Of the 21 reported cases including the present one, 18 cases were seen in the elderly with a mean age of 70 years and 3 cases in younger patients with mean age of 37 years.1,2,3,5,6,7,8,9 Our patient was the youngest to be affected at the age of 27 years. Another important finding seen among the elderly was the association of adenocarcinoma, which was not seen in the younger patients1,2,3,5,6,7,8,9 Table 1. This observation emphasizes the importance of long-term follow-up needed in younger individuals when diagnosed with gastric serrated adenoma.
|
References |
Total number of gastric serrated adenoma reported |
Serrated adenoma associated with carcinoma |
Age/average age |
|---|---|---|---|
|
7 |
6 |
73.3 |
|
|
Msakni I et al.1 |
1 |
0 |
50 |
|
Hasuo et al.7 |
1 |
1 |
67 |
|
Koklu et al.8 |
1 |
0 |
37 |
|
Kwon et al.9 |
9 |
7 |
67 |
|
Rubio et al.3* |
1 |
1 |
57 |
|
Divya et al.† |
1 |
0 |
27 |
*Case of Lynch syndrome. †Present case
According to the literature, the most common location of this neoplasm is in the cardia of the stomach.5 Kwon et al. described that the serrated adenoma of cardia has an increased risk of malignant transformation.9 The next common site of serrated adenoma is the body of the stomach, followed by the lesser curvature.5 Ours is the first case reported in the antrum of the stomach. Though this is a common site for adenomas, in general, it is a rare site for serrated adenoma.1
The Ki-67 IHC staining on the first case of serrated adenoma with an invasive component reported by Rubio showed an intense and continuous pattern in the dysplastic cells and superficial foveolar epithelium.2 The Ki-67 on the subsequent case also showed identical staining patter.5 Serrated adenoma in our case did not exhibit any associated invasive carcinoma, and Ki-67 staining was of intermitted pattern at the subepithelial glands and the lining epithelium Figure 2. This staining pattern was identical to that of serrated adenoma described by Ishiguro et al. They identified 3 characteristic Ki-67 staining patterns for regenerative polyps, serrated adenomas, and adenomatous polyps. Continuous and intense staining of the base and middle glands, intermittent staining pattern of the depressed part of superficial epithelium and continuous staining of all cells in the tumor glands were seen in regenerative polyps, serrated adenomas and adenomatous polyps, respectively.10 Based on the histomorphology and Ki-67 staining pattern, our case was a pure serrated adenoma without any invasive component.
Rubio and Björk in recent case report concluded that the serrated adenoma of the stomach follows the same pathway of progression to carcinoma as that of tubular, villous adenoma.3 In respect to this Kwon et al. and Hasuo et al. observed that serrated adenomas were positive for Muc5AC, KRAS and Muc5AC, Muc6, Muc2, and P53 respectively, concluding that, serrated adenoma exhibited the gastric phenotype and followed the adenoma-carcinoma pathway.9,7 This makes serrated adenoma a premalignant condition warranting close follow-up.
Conclusion
Gastric serrated adenoma, a rare entity, has a higher risk of malignant transformation. Association of an invasive component with serrated adenoma is common in the elderly whereas pure serrated adenoma is common amongst the young, often detected incidentally. Ki-67 staining may help identify the presence or absence of an invasive component. Though serrated adenoma has not yet been included as a distinct entity in the WHO classification of the gastric adenomas, it needs to be identified separately and considered as a precancerous lesion.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Serrated adenoma of the stomach: Case report and literature review. World J Gastrointest Endosc. 2013;5:261-4.
- [Google Scholar]
- Further studies on serrated neoplasias of the cardia: A review and case report. Anticancer Res. 2007;27:4431-4.
- [Google Scholar]
- Superficially elevated-type serrated hyperplastic lesion of the stomach with minute adenocarcinoma. Dig Endosc. 2009;21:101-5.
- [Google Scholar]
- Gastric serrated adenoma polyp treated with endoscopic band ligation (with video) Surg Laparosc Endosc Percutan Tech. 2010;20:e204-5.
- [Google Scholar]
- Serrated adenoma of the stomach: A clinicopathologic, immunohistochemical, and molecular study of nine cases. Histol Histopathol. 2013;28:453-62.
- [Google Scholar]
- Charecteristic feature of serrated adenoma on the evidence of Ki-67 positive cell pattern. Stomach Intestine (Tokyo). 1998;33:851-4.
- [Google Scholar]




