

Translate this page into:
Role of ultrasonography in the diagnosis of gall-bladder carcinoma: A boon for low-resource settings
Address for correspondence: Dr. Sachin Khanduri, Department of Radiodiagnosis, Era's Lucknow Medical College and Hospital, Lucknow, Uttar Pradesh, India. drsachinrad@gmail.com
This article was originally published by Thieme Medical and Scientific Publishers Private Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Purpose: The present study was done with an aim to evaluate the usefulness of ultrasonography (USG) in early diagnosis of gall-bladder carcinoma for low-resource settings.
Materials and Methods: A total of 264 clinically suspicious cases were enrolled in the study. The patients underwent USG followed by computed tomography (CT). Histopathological specimens were obtained from 208 cases. Final diagnosis was confirmed histopathologically/CT. Sensitivity, specificity, positive predictive, and negative predictive values of USG were calculated.
Results: A total of 29 cases were confirmed as gall-bladder carcinoma, 58.6% were diagnosed at advanced stage (Stage III/IV). USG diagnosed 42 cases as neoplastic, however, 24 were true positive and 18 were false positive. USG was 82.8% sensitive and 92.5% specific. The positive and negative predictive values were 57.1% and 97.8%, respectively, diagnostic efficacy was 91.5%. 94.1% advanced stage gall bladder cancers were diagnosed correctly by USG. Sensitivity for early stages was promising (61.9%), however false positive was higher. Cost of USG was nearly five times lesser as compared to that of CT.
Conclusion: USG was a useful economical imaging modality for the screening of gall bladder cancer in low-resource settings, especially for advanced stages. However, for early stages too, it seemed useful. We recommend to encourage the use of USG in early detection of gall-bladder carcinoma in socially and economically disadvantaged settings.
Keywords
Advanced Stage
Early Stage
Gall-bladder carcinoma
Promising
Ultrasonography

Introduction
Gallbladder cancer is a notoriously rare though lethal malignancy with marked ethnic and geographical variations. The basis for this variance likely resides in differences in environmental exposure and intrinsic genetic predisposition to carcinogenesis. It is the most common malignancy of the biliary tract, representing 80%−95% of biliary tract cancers worldwide, according to autopsy studies.1 It ranks sixth among gastrointestinal cancers.2 Epidemiological studies in India report its prevalence to range from 0.1 to 3.7 per one 100,000 population for males to 0.3–8.9 per one 100,000 population for females.3 However, the magnitude of the problem could be huge especially in the endemic zones of North-east India (Western Bihar and Eastern Uttar Pradesh) where it is the third commonest malignancy of the alimentary tract.4,5
The presenting symptoms are typically vague so that its diagnosis commonly occurs at an advanced stage. The risk factors vary geographically and among ethnic groups. In most of the cases, the gallbladder cancer takes nearly 5–15 years to develop with progression of metaplsia to dysplasia, carcinoma in situ and finally to invasive cancer in that order.1 Not only the late diagnosis but lack of a serosa in gallbladder is also responsible for a relatively poorer prognosis with an overall mean survival of 6 months in patients with advanced gall-bladder carcinoma and a 5-year survival rate of 5%.6
The diagnosis of gall-bladder carcinoma is challenging in view of the absence of specific signs and symptoms. Generally, noninvasive techniques such as ultrasonography (USG) also have been stated to have a limited role in early stages.7 In doubtful cases or where USG suggests a resectable biliary malignancy, CT, magnetic resonance imaging (MRI) with magnetic resonance cholangiography and/or traditional cholangiography often provide additional information. However, complementary modalities are usually needed for accurate staging.8 However, with the evolution of high-resolution USG, not only the accuracy in the diagnosis of gall-bladder carcinoma has increased but it has also shown a remarkable accuracy in distinguishing neoplastic polyps and staging gall bladder cancer.9,10
Incidentally, in India, the endemic zones for gall bladder disease, i.e., Western Bihar and Eastern Uttar Pradesh have one of the lowest GDP and advanced noninvasive imaging infrastructure such as computed tomography (CT) and MRI are scarcely available, hence, convinced with the recent reports showing the usefulness of high resolution USG in the diagnosis and differentiation of gall-bladder carcinoma, the present study was planned with an eye to evaluate whether USG can be helpful in the early diagnosis of gallbladder cancer in low-resource settings.
Materials and Methods
The study was performed in accordance with the guidelines of Institutional Review Board. The study was carried out on 264 consecutive clinically suspected cases of acute/chronic cholecystitis/cholelithiasis presenting with abdominal pain, weight loss, fever, and jaundice. All the patients were subsequently subjected to USG evaluation. USG examination was performed using Voluson-P8 USG machine (GE Healthcare) by a clinically experienced radiologist, with more than 20 years of clinical experience performing sonographic examination. All sonographic examinations were performed independently. During examination, an intercostal/subcostal scan was performed using both low frequency (1.5–4.5 MHz) and high frequency (5–7 MHz) transducer using real-time, spatial compound imaging techniques, and speckle reduction techniques as well as with and without harmonic imaging as per technique described by Lee et al. 2017.10 Image analysis was performed by a senior consultant in the department. Analyses were based on the formal reports focusing on the presence of GB cancer and the stage of the GB cancer. Presence of mass-occupying lesion nearly filling or replacing the lumen, often directly invading the surrounding liver parenchyma, focal or diffuse asymmetric wall thickening were considered to be suggestive of gall-bladder carcinoma.11,12
All the patients subsequently underwent operative procedure/computed tomographic evaluation on a 384-slice helical scanner (Siemens Somatom Force). Triphasic scan was done using dosage 60–80 ml/kg body weight. The images were read using multiplanar reconstruction on a slice thickness of 0.625 mm. The USG scan was performed by a clinically experienced radiologist, however the CT image analysis was done by three experienced faculty members to reach at a conclusion. The person who analyzed the images was blinded to the CT and histopathological results. The final diagnosis was made on the basis of correlation of histopathological/computed tomographic findings.
The diagnostic efficacy of USG was calculated against final diagnosis in terms of sensitivity, specificity, positive and negative predictive values, and overall accuracy.
Data analysis
Data was analyzed using Statistical Package for the Social Sciences (SPSS) version 21.0. Fisher's exact test was used to compare the data. A P < 0.05 indicated a statistically significant association.
Results
Age of patients ranged from 30 to 70 years. Mean age of patients was 48.42 ± 12.26 years. Majority of patients were females (91.7%). There were only 22 (8.3%) males. All the patients (100%) presented with abdominal pain, fever (51.5%), weight loss (38.6%) and jaundice (33.3%) were the other common presenting complaints. On the basis of histopathological/CT evaluation, the diagnosis was confirmed as cholelithiasis in 212 (80.3%) cases, benign gall bladder lesions in 23 (8.7%) cases, and gall-bladder carcinoma in 29 (11.0%) cases. Out of 29 cases diagnosed as gall-bladder carcinoma, a total of 3 (10.3%) were stage I, 9 (31%) were stage II, 10 (34.5%) were stage III, and 7 (24.1%) were stage IV cancers Table 1.
|
Characteristic |
Statistic (%) |
|---|---|
|
Mean age±SD (years), range |
48.42±12.26 (30-70) |
|
Male:female |
22 (8.3):232 (91.7) |
|
Presenting complaints |
|
|
Abdominal pain |
264 (100) |
|
Weight loss |
102 (38.6) |
|
Fever |
136 (51.5) |
|
Jaundice |
88 (33.3) |
|
Final diagnosis (based on histopathology/CT evaluation) |
|
|
Cholelithiasis |
212 (80.3) |
|
Benign gall-bladder lesions |
23 (8.7) |
|
Gall-bladder carcinoma |
29 (11.0) |
|
Stage I |
3/29 (10.3) |
|
Stage II |
9/29 (31.0) |
|
Stage III |
10/29 (34.5) |
|
Stage IV |
729 (24.1) |
SD - Standard deviation; CT - Computed tomography
On the basis of USG evaluation, a total of 214 (81.1%) were diagnosed as cholelithiasis, 18 (6.8%) were diagnosed as benign lesions, and 42 (15.8%) were diagnosed as gall bladder cancer. Out of 42 cases diagnosed as gall-bladder cancer by USG, a total of 24 were confirmed as gall bladder cancer, however, among the remaining 222 cases ruled out for gall bladder cancer, 5 were confirmed as gall bladder cancer. Correspondingly, USG had a sensitivity, specificity, positive predictive and negative predictive value for the diagnosis of gall-bladder cancer was 82.8%, 92.3%, 57.1%, and 97.7%, respectively. The overall accuracy of USG for the diagnosis of gall-bladder cancer was 91.3%. On evaluating the stage-wise cancer detection rate, out of 12 confirmed cases in lower stages (I/II), USG could diagnose 8 (66.7%) cases whereas out of 17 confirmed cases in higher stages (III/IV), USG could diagnose 16 (94.1%) cases. Although the detection rate was higher for higher stages, this difference was not statistically significant (P = 0.130) Table 2.
|
Diagnosis |
n (%) |
|||||||
|---|---|---|---|---|---|---|---|---|
|
Cholelithiasis |
214 (81.1) |
|||||||
|
Benign lesions |
18 (6.8) |
|||||||
|
Gall-bladder cancer |
42 (15.9) |
|||||||
|
Diagnostic efficacy for the detection of gall-bladder cancer |
||||||||
|
TP |
FP |
FN |
TN |
Sensitivity |
Specificity |
PPV |
NPV |
Accuracy |
|
24 |
18 |
5 |
217 |
82.8 |
92.3 |
57.1 |
97.7 |
91.3 |
|
Stage-wise cancer detection rate (sensitivity) |
||||||||
|
Lower stages (Stage I/II) |
Higher stages (Stage III/IV) |
|||||||
|
HPE/CT confirmed |
USG confirmed |
Percentage sensitivity |
HPE/CT confirmed |
USG confirmed |
Percentage sensitivity |
|||
|
12 P=0.130 (Fisher exact test) |
8 |
66.7 |
17 |
16 |
94.1 |
|||
TP – True positive; FP – False positive; FN – False negative; TN – True negative; PPV - Positive predictive values; NPV - Negative predictive values; CT - Computed tomography; USG – Ultrasonography; HPE - Histopathological examination
The average cost of USG with contrast was Rs. 650(∼$10) per case whereas average cost of CT with contrast was Rs. 3300(∼$50) per case Figures 123.
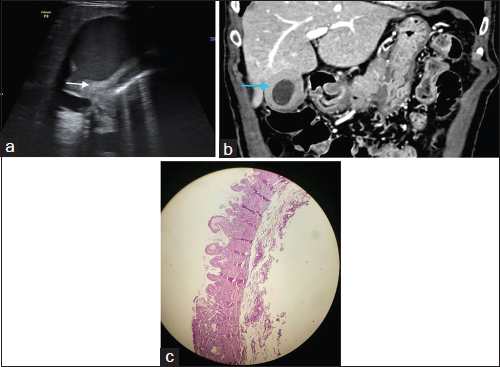
- (a) High-resolution transabdominal ultrasonography features in a 50-year-old female reveal diffuse circumferential gall bladder wall thickening (arrow) with evidence of echogenic foci within gall bladder lumen (sludge). (b) Coronal section computed tomography features of the same patient reveal circumferential gall bladder wall thickening (arrow) showing homogeneous postcontrast enhancement with mild pericholecystic fluid. (c) Imaging findings were suggestive of a benign pathology likely cholecystitis. Histopathology section from tissue obtained after surgery from the same patient shows epithelium lined by tall columnar cells with basally located nuclei. Focal area of epithelium shows sheets of lipid laden macrophages. Lamina propria is infiltrated by chronic inflammatory infiltrate comprising of lymphocytes and plasma cells. No malignant pathology is identified. The features were suggestive of cholecystitis with cholesterolosis
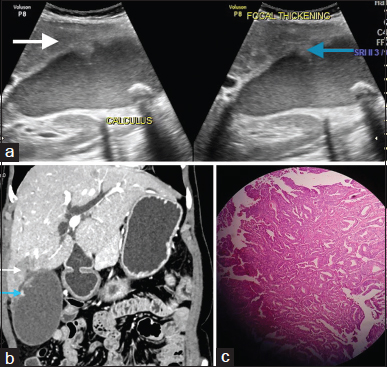
- (a) Transabdominal Ultrasonography features in a 35-year-old female reveal irregular wall thickening along anterior wall of gall bladder (blue arrow) with contiguous infiltration into adjacent segment V of liver (white arrow). An echogenic focus casting posterior acoustic shadow is noted within lumen (calculus) with additional evidence of multiple echogenic foci (sludge). (b) Coronal section computed tomography features of the same patient reveal focal irregular gall bladder wall thickening along its anterolateral aspect (blue arrow) with contiguous infiltration into adjacent segment V of liver (white arrow). The infiltration was also involving the common hepatic duct and cystic duct leading to bilobar intrahepatic biliary radicle dilatation (not seen). Imaging findings were suggestive of a malignant pathology likely adenocarcinoma of gall bladder. (c) Histopathology section from tissue obtained after surgery from the same patient shows glandular component as well as sheets of atypical cells having nuclear pleomorphism, high N:C ratio, coarse chromatin, eosinophilic cytoplasm with prominent nucleoli. The features were suggestive of a malignant pathology likely adenocarcinoma of gall bladder
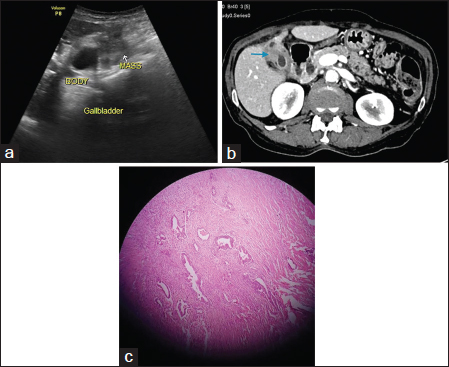
- (a) Transabdominal ultrasonography features of a 45-year-old male reveal diffuse gall bladder wall thickening with evidence of an ill-defined heterogeneously hypoechoic soft tissue mass lesion involving fundus and body of gall bladder. (b) Axial section computed tomography features reveal diffuse gall bladder wall thickening with evidence of an ill-defined heterogeneously enhancing mass lesion involving fundus and body of gall bladder (blue arrow). The lesion is abutting adjacent liver parenchyma with loss of fat planes. Imaging findings were suggestive of a malignant pathology likely adenocarcinoma of gall bladder. (c) Histopathology section from tissue obtained after surgery from same patient shows glandular component reaching up to the muscular layer lined by atypical cells having nuclear pleomorphism, high N:C ratio, coarse chromatin, eosinophilic cytoplasm with prominent nucleoli. Desmoplastic stroma is seen infiltrated by mild chronic inflammatory infiltrates comprising of lymphocytes and plasma cells. The features were suggestive of a malignant pathology likely adenocarcinoma of gall bladder
Discussion
Gall-bladder carcinoma is generally diagnosed at an advanced stage when medical intervention is restricted to palliation only. The reason for this late detection is the absence of specific signs and symptoms, reportedly low accuracy of primary noninvasive imaging techniques and unavailability/high cost of advanced imaging tools that might be helpful in diagnosing the disease. It is a pity that the regions having the highest burden of gall-bladder carcinoma are economically most disadvantaged and to think of using advanced diagnostic techniques such as CT and MRI is almost out of question. However, with the emergence of high-resolution USG, and subsequently its large-scale production has made it financially affordable even among the economically backward regions. Moreover, recent evidence has shown that HR-USG can be successfully employed in not only the diagnosis but also differentiation of gall-bladder cancer.9,10 This is a ray of hope for a low-resource setting where advanced diagnostic tools are beyond the reach of masses. Scanning at different frequencies has added value. Although we did not use both low- as well as high-frequency transducers for all the persons and it was most of the times on the clinical judgment of the performing ultasonologist. It was particularly useful in two cases of microlithiasis which could not be diagnosed on low frequency and required further exploration on high frequency.
In our study, we obtained a high accuracy of USG in diagnosing gall-bladder carcinoma (91.3%). Compared to the present study, Kim et al. 20159 in their study found HR-USG to be useful in characterization and differentiation of gall bladder polyps and different stages of gall-bladder carcinoma and reported the accuracy for different stage-differentiating categories to range from 65% to 92%. In the present study, we did not attempt to differentiate among different stages of gall-bladder cancer but rather attempted to differentiate gall-bladder carcinoma from benign lesions and cholelithiasis cases only. Bach et al. 199813 in their study also reported USG to be 94% sensitive in the detection of resectable gall-bladder lesions.
In our study, gall-bladder cancer was slightly overdiagnosed by HR-USG thus rendering its positive predictive value as 57.1% only. This positive predictive value is higher than that reported by Cho et al. 2009,14 who while using endoscopic USG reported a positive predictive value of 85%. The reason for relatively lower positive predictive value in the present study could be attributed to the difference in both technique as well as patient characteristics. In the present study, we performed transabdominal USG instead of endoscopic USG and took all the suspect cases whereas the referred study14 included patients with gall bladder polyps alone. However, in the study by Bach et al. 199813 similar to our study, USG was found to have 58% positive predictive value in detecting resectable gall-bladder carcinoma.
In the present study, overall sensitivity of HR-USG was 82.8%, though this sensitivity was lower for early stages (66.7%) as compared to higher stages (94.1%), yet an overall sensitivity rate was within a reasonable range (82.8%). Although this difference was not significant statistically yet owing to fewer number of cases in present study, the statistical power of the finding is limited, hence needs further exploration. It must be kept in mind that compared to findings in the present study earlier studies prior to the emergence of HR-USG have reported the sensitivity of USG to be quite poor (44%).7 In the present study, even the inclusion of cholelithiasis cases did not result in a poorer sensitivity as envisaged by some authors,15 thus indicating that USG crosses the barrier posed by cholelithiasis and enables to visualize the characteristic USG features of gall-bladder carcinoma more clearly. With the help of both low- and high-frequency transducers during high-resolution transabdominal sonography of the gallbladder, one can successfully delineate between the layers of the gallbladder wall that helps in getting a better image characterization,9 in the present study, utilization of this approach helped in increasing the sensitivity of USG to a great extent. In its consensus document, the Indian Council of Medical Research also recommends patient specific low-/high-frequency transducer use for the detection of gall-bladder carcinoma and proposes its accuracy to be as high as 90.5%.16 In the present study, we utilized a harmonic frequency modulation as suggested by Kim et al. 20159 and thus were able to determine the depth of tumor invasion in most patients as this technique enabled detailed visualization of the layers of the gall bladder, however, we must admit that this was the reason for slight overdiagnosis of gall-bladder carcinoma, thus resulting in relatively lower positive predictive value (57.1%). However, this approach was successful in visualizing deep-seated lesions efficiently, thus increasing the overall sensitivity.
The findings of present study showed that with the skillful use of USG in the detection of gall bladder cancer in low-resource settings, with a high sensitivity (82.8%), it can help in the identification of a large number of gall-bladder carcinoma cases in settings where advanced imaging tools such as CT and magnetic resonance are not available. USG was also an economical tool for screening and detection of gall-bladder cancer and minimizing the role of more costly imaging modalities such as CT. Moreover, a high sensitivity (66.7%) for early stage and resectable cases as observed in present study also shows that USG can help in identifying a large proportion of those cases which otherwise remain undiagnosed and might have a favorable prognosis. Although a low positive predictive value is one of the issues that needs to be settled with continuous exploratory studies for characterizing more specific features that might help in reducing the burden of false positivity yet despite this low positive predictive value, the screening potential of USG cannot be ruled out, more so, in an underprivileged population.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Epidemiology and molecular pathology of gallbladder cancer. CA Cancer J Clin. 2001;51:349-64.
- [Google Scholar]
- Consolidated Report of the Population Based Cancer Registries of the National Cancer Registry Programme (1990-1996) New Delhi: ICMR Publication; 2001. p. :52.
- [Google Scholar]
- Primary carcinoma of the gall bladder: A review of a 16-year period at the university hospital. J Surg Oncol. 1985;28:32-5.
- [Google Scholar]
- Carcinoma of the gallbladder: A retrospective review of 99 cases. Dig Dis Sci. 2001;46:1145-51.
- [Google Scholar]
- Gallbladder carcinoma: Radiologic-pathologic correlation. Radiographics. 2001;21:295-314.
- [Google Scholar]
- Ultrasonography in carcinoma of the gallbladder. Diagnostic difficulties and pitfallsActa Radiol. 1987;28:715-8.
- [Google Scholar]
- Diagnostic imaging of carcinomas of the gallbladder and the bile ducts. Acta Radiol. 2006;47:345-58.
- [Google Scholar]
- High-resolution sonography for distinguishing neoplastic gallbladder polyps and staging gallbladder cancer. AJR Am J Roentgenol. 2015;204:W150-9.
- [Google Scholar]
- Diagnostic accuracy of transabdominal high-resolution US for staging gallbladder cancer and differential diagnosis of neoplastic polyps compared with EUS. Eur Radiol. 2017;27:3097-103.
- [Google Scholar]
- Sonographic features of carcinoma of the gallbladder. Gastrointest Radiol. 1981;6:169-73.
- [Google Scholar]
- Gallbladder cancer: Can ultrasonography evaluate extent of disease? J Ultrasound Med. 1998;17:303-9.
- [Google Scholar]
- Hypoechoic foci on EUS are simple and strong predictive factors for neoplastic gallbladder polyps. Gastrointest Endosc. 2009;69:1244-50.
- [Google Scholar]
- Diagnostic imaging of early gallbladder cancer: Retrospective study of 53 cases. World J Surg. 1999;23:708-12.
- [Google Scholar]
- Consensus Document for Management of Gallbladder Cancer Prepared as an Outcome of ICMR Subcommittee on Gallbladder Cancer. Div. of Noncommunicable Diseases New Delhi: Indian Council of Medical Research; 2014. editors. Available from: http://www.icmr.nic.in/guide/cancer/GallBladder/GALLBLADDERCANCER.pdf
- [Google Scholar]




