

Translate this page into:
Rib tumors: A ten-year institutional study
 DNB, Ashini Shah1MD, Priti Trivedi1MD
DNB, Ashini Shah1MD, Priti Trivedi1MD
* Corresponding author: Amisha Gami, MD, Department of Oncopathology, The Gujarat Cancer and Research Institute, Ahmedabad, India. docamishamehta@yahoo.co.in
-
Received: ,
Accepted: ,
How to cite this article: Paul JS, Sunita S, Gami A, Gandhi J, Shah A, Trivedi P. Rib tumors: A ten year institutional study. Asian J Oncol. 2024;10:7. doi: 10.25259/ASJO-2022-50-(408)
Abstract
Objectives
The primary aim of this study was to study the demography and frequency distribution of the various rib tumors. The treatment modality offered and patient outcomes were also recorded wherever available.
Material and Methods
A ten year data was retrieved from the hospital registry from 2011-2021. Inclusion criteria were all patients with any tumors in the rib. Those patients who did not have a histological diagnosis and those having a chest wall mass and secondary involvement of the ribs were excluded.
Results
Out of 72 cases of rib tumors, 25 were diagnosed as Ewing Sarcoma, 22 Chondrosarcoma cases, 10 Multiple myeloma/plasmacytoma cases, 9 Osteosarcoma cases, rest 1 case each of Non Hodgkin Lymphoma, Brown tumor, Enchondroma, Osteochondroma, Clear cell sarcoma and metastases.
Conclusion
In this study the most common primary malignant tumor of the ribs in adults was Chondrosarcoma (41.1%) and in pediatric & young adolescent age group (upto 18yrs) it was Ewing sarcoma (76.1%)
Keywords
Rib tumors
Ewing Sarcoma
Chondrosacroma
Osteosarcoma

INTRODUCTION
Ribs are a part of the axial skeletal system. The axial skeleton, being rich in red marrow, makes it vulnerable to metastatic tumors.[1] Ribs also have costochondral junctions which could be the source of origin of cartilaginous tumors. Primary bone tumors of the ribs are rare, comprising only about 3–8% of bone tumors.[2] Among the rib tumors, literature search says that benign tumors are the most common primary tumors, and among malignant tumors involving the ribs, metastatic tumors are more common than primary tumors.[3] A study was conducted at a tertiary cancer center in the western part of India to study the most common rib tumors.
MATERIAL AND METHODS
A retrospective descriptive study was conducted in a tertiary cancer institute in Western India by retrieving ten year data from the hospital registry, from 2011 to 2021, of all patients who visited the ortho–oncology department of the Institute and had tumors in the ribs. Inclusion criteria were all patients with any tumor in the rib. Those patients who did not have a histological diagnosis were excluded from the study. Also, patients with a chest wall mass and secondary involvement of the ribs were excluded. The treatment taken and patient follow-up was recorded wherever available. Immunohistochemical analysis was performed in some of the cases on formalin fixed paraffin embedded tissue by fully automated machine (Ventana Benchmark XT) using monoclonal antibodies.
RESULTS
A total of 72 patients were enrolled in the study after excluding patients without a histological diagnosis. The age range was from 5 to 75 years with a median age of 30 years. Male to female ratio was 51:21, and the ratio of benign to malignant tumors was 1:23 (3 benign and 69 malignant). The most common ribs involved were the fourth and seventh ribs, and the left side was found to be more commonly involved than the right side. All three benign tumors had presented with a swelling.
DISCUSSION
Ribs are an uncommon site for primary bone tumors. Fortunately, most of them, especially chondroid lesions, occur in the anterior aspect which make them more visible when not painful and hence call for attention.[4] Rib tumors can be benign or malignant, and hence an X ray as a primary investigation followed by Computed Tomography (CT), Magnetic Resonance Imaging (MRI) or Positron Emission Tomography (PET) scan may be needed. A Jamshidi (J) needle biopsy is undertaken as per the radiological diagnosis, planning it in such way that the tract may be excised in case it turns out to be malignant. Benign tumors are excised if symptomatic and wide excision is performed in malignant tumors.[5]
Benign tumors
A study by Cakmak et al. reported benign rib tumors in 63% of their patients,[6] while our study had 4% of benign tumors. The high incidence of malignant tumors in our study is attributed to our institute, being a tertiary cancer referral center, where all the benign tumors are filtered out before reaching the institute. The three benign tumors encountered in our study were osteochondroma, enchondroma, and brown tumor. Refer to Table 1 for the list of benign tumors obtained in our study.
| Sl. no. | Diagnosis | Total cases (n) (%) | Age (year) | Sex | Laterality and ribs involved |
|---|---|---|---|---|---|
| 1 | Osteochondroma | 1 (1.3%) | 5 | M | Bilateral 4th and 5th ribs |
| 2 | Enchondroma | 1 (1.3%) | 38 | M | Left 6th rib |
| 3 | Brown tumor | 1 (1.3%) | 35 | F | Left side 5th rib |
M: Male, F: Female
Brown tumor
The recorded incidence of brown tumor is 3% in cases of primary hyperthyroidism.[7] Our 35-year-old patient presented with a painful swelling in the rib which was biopsied and reported to be a giant cell–rich lesion, raising the possibility of a brown tumor. Serum Parathyroid hormone (PTH) was found to be toward the upper limit of normal 51.4 picogram (pg). Normal levels were in the range 10–55 picograms/mL. On further investigation, a parathyroid adenoma was discovered, which confirmed the diagnosis. Treatment of the primary etiological factor should be done before removal of the brown tumor. After resection of the pathological parathyroid, the bone lesion tends to resolve spontaneously.[7]
Osteochondroma
The patient with a rib osteochondroma was a five year-old child with polyostotic osteochondroma involving multiple bilateral ribs and humerus. The lesion in question was excised from the rib with a suspicion of malignant transformation; however, histopathology confirmed osteochondroma without any malignant transformation. The estimated risk of malignant transformation of polyostotic osteochondroma is 5–25% with clinic-radiological signs and symptoms of sudden rapid progression, cartilage cap of more than 2 cm thickness, and infiltration into soft tissue.[8] Osteochondromas commonly occur around the knee joint with very rare involvement of the ribs. However, in patients with hereditary polyostotic osteochondromatosis, ribs are involved in 55% of the cases.[9] These lesions can be left alone for follow-up if asymptomatic, however, need to be excised if they cause local symptoms or malignant transformation.
Enchondroma
The patient with enchondroma was a 38-year-old male patient with involvement of the left sixth rib. The radiology was suggestive of a chondroid lesion, possibly enchondroma. The patient was biopsied elsewhere and we had received slides for review which confirmed the diagnosis of enchondroma. The patient was lost to follow-up. Enchondromas are believed to be the second most common rib tumors after fibrous dysplasia, accounting for about 15–20% of benign rib tumors.[9] These tumors are easy to identify radiologically when they have the classical calcification and are limited to the bone.
Malignant tumors
Of the malignant rib tumors, the incidence has varied in various studies. However, metastasis and myeloma are believed to be the most common.[10] Our study only had one out of 69 malignant metastatic tumors from ovarian adenocarcinoma. Ribs are believed to be the third most common site for metastasis after spine and femur.[10] Though metastatic tumors are the most common malignant tumors, our study is probably skewed as the rib tumor would not have been the presenting symptom. The patients probably had multiple secondaries, and the other sites have been biopsied rather than the rib resulting in such a low incidence of metastatic rib tumors. The list of malignant tumors in our study is shown in Table 2.
| Sl. no. | Diagnosis | Total cases (n) (%) | Age range (year) | Sex (M:F) |
|---|---|---|---|---|
| 1 | Ewing sarcoma | 25 (36.2%) | 5–27 | 21:4 |
| 2 | Chondrosarcoma | 22 (31.8%) | 17–75 | 16:6 |
| 3 | Plasmacytoma | 10 (14.5%) | 35–68 | 6:4 |
| 4 | Osteosarcoma | 9 (13.0%) | 16–52 | 4:5 |
| 5 | Non-Hodgkin lymphoma | 1 (1.4%) | 40 | Male |
| 6 | Clear cell sarcoma | 1 (1.4%) | 8 | Male |
| 7 | Metastatic adenocarcinoma | 1 (1.4%) | 32 | Female |
| 8 | Non-Hodgkin lymphoma | 1 (1.4%) | 40 | Female |
Ewing sarcoma
Ewing sarcoma is known to comprise about 5–10% of the malignant rib tumors.[11] On the other hand, we found Ewing sarcoma to be the most common malignant rib tumor comprising 36.2 % of malignant tumors. The age group ranged from 5–27 years. In a study by Grier et al., only 13% of Ewing sarcoma involved the ribs, which suggested that the ribs are not a very common site for primary Ewing sarcoma.[12] Though the literature states that 5–10% of malignant rib tumors are Ewing sarcoma, we had 36.2% of these cases, which highlighted the high incidence of these tumors in the ribs. The gross picture of a case of Ewing sarcoma of the rib is shown in Figures 1a and 1b.
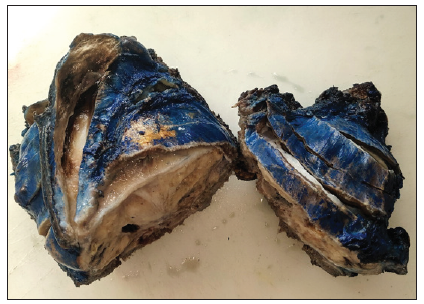
- Ewing sarcoma rib.
- Ewing sarcoma rib.
Of the 25 cases of Ewing sarcoma in our study, all of them had Cluster of differentiation 99 (CD 99)-positive staining on Immunohistochemistry (IHC) with or without Friend Leukemia Integration 1 transcription factor (FLI 1) positive staining. One patient with a histological diagnosis of a malignant round cell tumor and suspected to be Ewing sarcoma turned out to be non-Hodgkin lymphoma, which highlighted the role of immunohistochemistry in all cases irrespective of morphology and clinical presentation. Four patients developed local recurrence following chemotherapy and surgery, and nine patients developed metastasis. Metastasis was in the lungs in four cases, bone in three cases, and pleura in one case. Four cases showed both lung and bone metastases. The overall local recurrence and metastatic rate was 11/25 (44%) with two cases having both local recurrence and metastasis. One patient was lost to follow-up, while the other 24 received combination therapy in the form of chemotherapy and surgery with or without radiotherapy. The treatment response and modalities in Ewing sarcoma are shown in Table 3.
| Ewing sarcoma (Total 25 cases) | Parameter | No. of cases |
|---|---|---|
| Residual tumor in resected specimen (10) | >50% | 0 (0.00) |
| 10–50% | 2 (0.20) | |
| 1–10% | 5 (0.50) | |
| <1% | 3 (0.30) | |
| Treatment modality | Chemotherapy | 7 (0.28) |
| Chemotherapy and surgery | 6 (0.24) | |
| Chemotherapy and RT | 5 (0.20) | |
| Surgery and RT | 2 (0.08) | |
| Chemotherapy, surgery, and RT | 4 (0.16) | |
| Not available | 1 (0.04) |
RT: Radiotherapy
According to American Cancer Society, the overall five year survival rate for localized Ewing sarcoma is 70%, and patients with metastatic disease have a five year survival rate of 15–30%.[13] Longest follow-up in our study with recurrence and metastases was three years and nine months, and without recurrence was two years and three months.
Chondrosarcoma
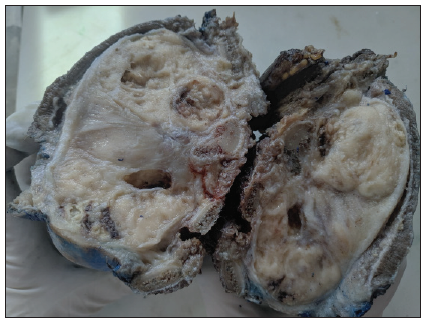
Chondrosarcoma accounts for 11–16% of primary malignant rib tumors in adults.[14] The common sites are shoulder, pelvis, thoracic wall, and rarely base of the skull. In the thorax, there is a predilection for the upper five ribs of anterior chest wall and in close association with costochondral junction.[10] In our study, the incidence was 30.9%, being the second most common malignant rib tumor after Ewing sarcoma. The age group ranged from 17–70 years with a male to female ratio of 2.6:1. T2 was the most common stage of presentation comprising 45 % of chondrosarcoma and Grade 2 was the most common grade. A total of three patients had lung metastasis of which one had metastasis at presentation and the other had associated local recurrence. In our study, metastatic sites included the lungs, liver, abdominal wall, and peritoneum. All patients received treatment in the form of surgery with or without chemotherapy or radiotherapy. According to a study by King et al., the ten year survival rate after wide resection was 96.4% as compared with 65.4% for those who underwent only local excision.[15] Longest follow-up of a chondrosarcoma case available without recurrence in our study was five years.
The gross picture of a case of rib chondrosarcoma is shown in Figures 2a and 2b. The histological grade, stage, tumor extension, and treatment modalities of chondrosarcoma cases in our study are shown in Table 4.
- Chondrosarcoma rib.

- Chondrosarcoma rib.
|
Chondrosarcoma (Total 22 cases) |
Parameter | No. of cases |
|---|---|---|
| Histological grade | Grade 1 | 4 (0.18) |
| Grade 2 | 16 (0.72) | |
| Grade 3 | 2 (0.09) | |
| Stage at presentation | T1 | 8 (0.36) |
| T2 | 10 (0.45) | |
| T1M1b | 1 (0.04) | |
| Not available | 3 (0.13) | |
| Tumor extension | Limited to bone | 11 (0.50) |
| Extends to soft tissue | 9 (0.40) | |
| Not available | 2 (0.09) | |
| Treatment modality | Surgery | 8 (0.36) |
| Surgery and RT | 3 (0.13) | |
| RT | 3 (0.13) | |
| Chemotherapy | 1 (0.04) | |
| Chemotherapy and RT | 1 (0.04) | |
| Not available | 6 (0.27) |
RT: Radiotherapy
Osteosarcoma
Osteosarcoma has a bimodal age of presentation and is the most common primary malignant bone tumor in children. Our study recorded an incidence of 12.6 % of rib tumors in the age group of 16–52 years. Of the osteosarcomas, ribs are a rare site to occur, and the reported incidence of primary rib osteosarcoma is only about 1–3%.[16] Osteosarcoma is a morphological diagnosis and usually does not need immunohistochemistry for confirmation in a classical clinical background and supported by classical radio imaging findings. However, we performed IHC in two cases, where one was telangiectatic osteosarcoma, just for confirmation. The other was a 52-year-old female with a 12 cm mass who had a high-grade sarcoma. Only focal osteoid-like material was seen, Special AT- rich sequence - binding protein 2 (SATB2) positivity confirmed the diagnosis. Longest follow-up of an osteosarcoma case in our study without recurrence was three years and one month. In our study, two cases had metastases, one at the time of diagnosis and one after one year of diagnosis. Metastatic sites included the lungs and the abdomen.
Though pathologists have a fancy to subclassify them as chondroblastic, osteoblastic, or fibroblastic, they do not actually have any prognostic or therapeutic implications. However, telangiectatic osteosarcomas are more aggressive and less responsive to treatment. Rib is an uncommon site for primary osteosarcoma, and a rib lesion should raise the suspicion of the lesion in question being a metastatic osteosarcoma. The histological subtype, treatment response, and treatment modalities in osteosarcoma cases in our study are shown in Table 5.
|
Osteosarcoma (Total 9 cases) |
Parameter | No. of cases |
|---|---|---|
| Histological subtype | Chondroblastic | 4 (0.44) |
| Osteoblastic and fibroblastic | 2 (0.22) | |
| Osteoblastic and chondroblastic | 2 (0.22) | |
| Telangiectatic | 1 (0.11) | |
| Residual tumor in resected specimen (3) | >50% | 1 (0.33) |
| <50% | 2 (0.66) | |
| Treatment modality | Chemotherapy | 2 (0.22) |
| Surgery | 1 (0.11) | |
| Surgery, chemotherapy, RT | 1 (0.11) | |
| Surgery, chemotherapy | 2 (0.22) | |
| Not available | 3 (0.33) |
RT: Radiotherapy
Multiple myeloma and plasmacytoma
Multiple myeloma is a malignant clonal neoplasm of B lymphocyte plasma cells typically presenting in the fifth and sixth decades. According to a study by Zarqane et al., the ribs are the second most common site of involvement in multiple myeloma, which occurred in 45–50% of patients.[10] Plasmacytomas are rare, and accounts for only 4% of plasma cell neoplasms and presents between fourth and sixth decades.[17] In our study, the incidence rate of plasma cell neoplasm was 14% in which seven were plasma cell myeloma cases and three were solitary plasmacytomas.
Non-Hodgkin lymphoma
In our study, one case of lymphoma with involvement of the ribs was detected in a 40-year-old female patient. It was confirmed with IHC as a non-Hodgkin lymphoma, large B cell lymphoma. The patient had concurrent lymph nodes and a paraspinal mass at the same time, both of which were not sampled. Patient had a recurrence in the left inguinal node eight years later and it was diagnosed as non-Hodgkin lymphoma – diffuse large B cell lymphoma – germinal center B type. Secondary bone lymphomas are found in around 15% of disseminated lymphomas.[18] This is defined as lymphoma involving the bone with nodal disease occurring within six months or secondary lymphoma involving the bone at least six months after diagnosis. The most common sites are spine, bony pelvis, skull, ribs, and facial bones.[19]
Clear cell sarcoma
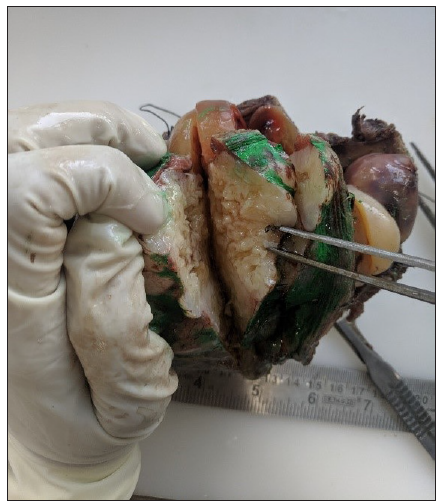
Clear cell sarcoma (malignant melanoma of soft tissues) is a very rare soft tissue neoplasm comprising 1% of all musculoskeletal sarcomas. Metastasis of malignant melanoma to bone is not uncommon, but primary clear cell sarcoma of the bone is an extremely rare neoplasm.[20] In our study, one case of rib clear cell sarcoma was diagnosed in the lateral aspect of sixth and seventh ribs in an 8-year-old male child. The gross picture of clear cell sarcoma of the rib is shown in Figure 3. It was confirmed with immunohistochemistry Soluble 100% (S100), SRY - box transcription factor 10 (S0X 10), and Human melanoma black 45 (HMB 45), which were strongly positive.
- Clear cell sarcoma rib.
Drawbacks or weakness of the study
As this study was carried out in a tertiary cancer center, the proportion of malignant tumors is more than that of the benign tumors. In our study, only one case of metastases to the rib was found which was in contrast with other studies where metastatic tumors to the ribs were more common than primary.
CONCLUSION
Primary malignant bone tumors are rare and comprise 3–5% of all tumors in childhood and less than 1% in adults, of which the tumors involving the ribs are rare.[21] A comprehensive study exclusive of the rib gives an account of the demography of the tumors and frequency of the individual tumors. This study will give a bird’s eye view on the differentials of rib tumors. It also makes us aware that when an osteosarcoma of the rib is detected, one should rule out metastatic osteosarcoma. Though our study shows Ewing sarcoma and chondrosarcoma as the most common tumors in children and adults, respectively, the overall data suggest that benign tumors are at least as common as malignant ones.
Ethical approval
The research/study approved by the Institutional Ethics Committee OR IRB at The Gujarat Cancer and Research Institute, Reference number is IRC/2023/P-18, dated 25/01/2023.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
REFERENCES
- Bone metastases: An overview. Oncol Rev. 2017;11:321.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Keep your eyes on the ribs: the spectrum of normal variants and diseases that involve the ribs. Radio Graphics. 1999;19:1125-42.
- [CrossRef] [PubMed] [Google Scholar]
- Primary tumors of the ribs; experience with 78 patients. Interact Cardiovasc Thorac Surg. 2009;9:251-4.
- [CrossRef] [PubMed] [Google Scholar]
- Brown tumor of the rib as a first presentation of primary hyperparathyroidism: Report of three cases and literature review. Thorac Cancer. 2013;4:474-8.
- [CrossRef] [PubMed] [Google Scholar]
- MR imaging of solitary osteochondromas: Report of eight cases. AJR Am J Roentgenol. 1987;149:557-60.
- [CrossRef] [PubMed] [Google Scholar]
- The spectrum of rib neoplasms in adults: A practical approach and multimodal imaging review. AJR. 2020;215:165-77.
- [CrossRef] [PubMed] [Google Scholar]
- Localized Ewing tumor of bone: Final results of the cooperative Ewing’s Sarcoma Study CESS 86. J Clin Oncol. 2001;19:1818-29.
- [CrossRef] [PubMed] [Google Scholar]
- The Ewing family of tumors. Ewing’s sarcoma and primitive neuroectodermal tumors. Pediatr Clin North Am. 1997;44:991-1104.
- [CrossRef] [PubMed] [Google Scholar]
- SEER cancer statistics review, 1975–2017. Bethesda, MD: National Cancer Institute; 2020.
- A single-institutional, multidisciplinary approach to primary sarcomas involving the chest wall requiring full-thickness resections. J Thorac Cardiovasc Surg. 2001;121:48-60.
- [CrossRef] [PubMed] [Google Scholar]
- Primary chest wall tumors: Factors affecting survival. Ann Thorac Surg. 1986;41:597-601.
- [CrossRef] [PubMed] [Google Scholar]
- Osteogenic sarcoma of the rib: a case presentation and literature review. Spine (Phila Pa 1976). 2003;28:E74-E77.
- [CrossRef] [PubMed] [Google Scholar]
- Lymphoma of bone, muscle, and skin: CT findings. AJR Am J Roentgenol. 1992;159:805-9.
- [CrossRef] [PubMed] [Google Scholar]
- Radiological manifestations of skeletal lymphoma. Curr Probl Diagn Radiol. 2009;38:228-36.
- [CrossRef] [PubMed] [Google Scholar]




