

Translate this page into:
The psycho-social impact of cancer treatment on the caregivers of the patients
Corresponding author: Dr. Subbiah Shanmugam, Department of Surgical Oncology, Government Royapettah Hospital, Chennai, Tamil Nadu, India. subbiahshanmugam67@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Shanmugam S, Jebasingh AV, Singodiya S, The psycho-social impact of cancer treatment on the caregivers of the patients. Asian J Oncol. 2024;10:16. doi: 10.25259/ASJO_5_2024
Abstract
Objectives
The incidence of cancer cases shows an increasing trend over the past two decades owing to several factors, such as increased life expectancy, aging population, behavioral, environmental, and occupational risk factors, and more. Consequently, a greater number of people are expected to take the role of principal caregivers in the near future. Cancer treatment can have a multifaceted impact on the quality of life and psychological well-being of not only the patients but also their families. Caregivers are expected and required to provide complex care and support for which they are neither prepared nor trained. The reports of feeling overwhelmed and stressed are high when the demands placed on them exceed their resources, resulting in a negative effect on the overall well-being of the caregivers, including the patients themselves. The impact covers a wide spectrum of emotional, physical, financial, social, cognitive, spiritual, and work-related effects.
Material and Methods
This is a cross-sectional study conducted (for over three months from May to July 2023) among the caregivers accompanying cancer patients attending a tertiary care hospital in a South Indian metropolitan city. All the adult caregivers of patients diagnosed with cancer at least two to six months before the time of the study were considered as the study population. A systematic random sample was applied to recruit a convenient sample of 150 caregivers, maintaining the enrollment of only one caregiver per patient. Sociodemographic details of the patients and their caregivers were collected. The Zarit Burden Interview (ZBI) based on a Likert scale was implemented to collect relevant data related to both the cancer patient and the family caregiver.
Results
Of the total 150 cancer patients, the most common type of cancer among the patients was head and neck (63, 42%), followed by cancers of the female reproductive system (44, 29.3%) and breast (24, 16%). Nearly 47% of caregivers were children of cancer patients, while 35.3% were spouses. Significantly higher burden scores on the “emotional strain” and “financial/physical strain” domains were observed among female caregivers. Higher burden scores on the “self-criticism” domain were independently associated with a shorter caregiver-patient contact time. Significantly higher burden scores on the “self-criticism” and “time/dependence” domains were observed among employed caregivers. Higher levels of burden on the “financial/physical strain” domain were reported by unemployed caregivers. Significantly higher burden scores on the “uncertainty” domain were observed among older caregivers and caregivers who were parents or spouses of the patients.
Conclusion
Caregiving impacts the physical, emotional, financial, and social aspects of the caregiver’s life. They adopt active coping strategies to overcome the impacts of caregiving. A majority of the caregivers experienced mild to moderate burden, while most scored low on quality of life. Attention to concerns and the psychological well-being of caregivers may improve the overall scenario.
Keywords
Psychosocial impact
Zarit burden interview
Caregiving

INTRODUCTION
The incidence of cancer cases has shown an increasing trend over the past two decades owing to several factors, such as increased life expectancy, aging population, behavioral, environmental, and occupational risk factors, and more. Consequently, a greater number of people are expected to take the role of principal caregivers in the near future. Cancer treatment can have a multifaceted impact on the quality of life and psychological well-being of not only the patients but also their families. Caregivers are expected and required to provide complex care at home for which they are neither prepared nor trained. The reports of feeling overwhelmed and stressed are high when the demands placed on them exceed their resources, resulting in a negative effect on the overall well-being of the caregivers. The impact covers a wide spectrum of emotional, physical, financial, social, cognitive, spiritual, and work-related effects. The impact on the psychological domain of quality of life appears as emotional distress, feelings of guilt and helplessness, and difficulty in coping with the caregiving roles. Physical impact may include fatigue, physical strain, and neglect of personal health; financial impact includes direct and indirect costs of the illness (cancer) in the form of medical expenses and wage loss due to quitting work in order to provide care (work impact); social impact appears in the form of isolation, loneliness, and strained relationships; cognitive impact can be seen as a decision-making pressure and the need to be constantly vigilant of the patient’s symptoms, medications, and so on; and spiritual impact such as questioning one’s own religious beliefs and seeking meaning in the current suffering has the potential to make the caregivers overwhelmed. In view of this, this study was planned to assess the psychosocial impact of cancer treatment on the caregivers of cancer patients.
Objectives
-
1.
To assess the psychosocial impact of cancer treatment among the caregivers of cancer patients using the ZBI.
-
2.
To determine the factors affecting the quality of life and psychosocial well-being of caregivers of cancer patients.
MATERIAL AND METHODS
This is a cross-sectional study conducted among the caregivers accompanying cancer patients attending a tertiary care hospital in a South Indian metropolitan city from May to July 2023. All the adult caregivers of patients diagnosed with cancer at least two to six months before the time of the study were considered as the study population. The caregivers who were willing to participate and give informed oral consent were included in the study.
A systematic random sample was applied to recruit a convenient sample of 150 caregivers, maintaining the enrollment of only one caregiver per patient. Participant anonymity and confidentiality of their personal information were ensured by removing identification details from the data before analysis. The data collected were entered, cleaned, coded, and analyzed in Microsoft Excel 2010, and inferential statistics were performed using IBM SPSS version 21.
Sociodemographic details of the patients and their caregivers were collected. The Zarit Burden Interview (ZBI), based on the Likert scale, was implemented to collect relevant data related to both the cancer patient and the family caregiver. This is a 22-item instrument that includes the items most frequently mentioned by caregivers as problem areas in providing care for patients with chronic mental illness (http://www.healthcare.uiowa.edu/igec/tools/caregivers/burdenInterview.pdf). It explores the negative physical, mental, social, and economic impacts of caregiving on the life of the caregiver. The responses are rated on a Likert scale of 0 (never) to 4 (almost always), with a total score of 0–88. Higher scores indicate higher levels of caregiver burden or distress. The caregivers’ responses to each component of the ZBI were recorded as Likert-based responses from 0 to 4, and the arithmetic value of each response was considered for analysis. Domain-wise totals were calculated for the five domains, viz “financial/physical strain,” “time/dependency strain,” “emotional strain,” “uncertainty,” and “self-criticism.” A total score was calculated for each caregiver as the sum of all their responses. Based on this total score, the caregivers were classified as having “Little or no burden” (total score 0–20), “Mild to moderate burden” (total score 21–40), “Moderate to severe burden” (total score 41–60), and “Severe burden” (total score 61–88). The most common response (Statistical Mode) among all the caregivers was calculated for each question. The factors determining the domain scores and total scores were identified.
RESULTS
This study enrolled a total of 150 cancer patients and their caregivers (one caregiver per patient). The cancer patients were aged between 17 and 75 years, with a mean age of 54.64 ± 17.21 years, a majority of them aged between 51 and 70 years (47.06) [Figure 1]. A male predominance was noticed among the cancer patients (85, 56.7%) [Figure 2].
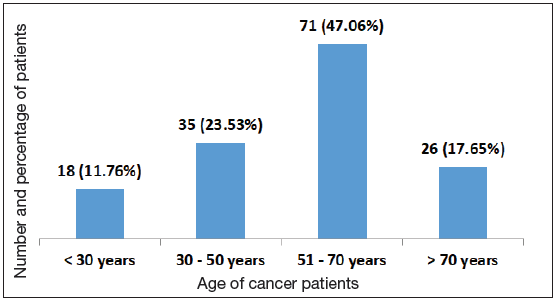
- Distribution of cancer patients based on their age (n = 150).
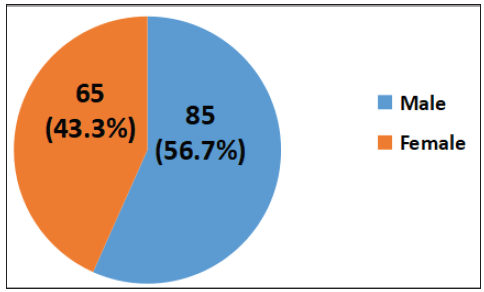
- Gender-wise distribution of the cancer patients (n = 150).
Among the cancer patients, 97 (64.7%) were married, 35 (23.5%) widows, and 18 (11.8%) unmarried. Most of the patients were educated up to high school (62, 41.2%), nearly another quarter (35, 23.5%) were graduates, and more than a third (53, 35.3%) were illiterate. The distribution of cancer patients based on their occupation was similar to that based on education, viz most patients (60, 40%) were unemployed, 59 (39.3%) unskilled workers, and 31 (20.6%) skilled workers. The monthly income of the patients ranged between INR 5000 and INR 30,000, with 97 (64.7%) having a monthly income of INR 10,000–20,000.
The patients traveled an average distance of 72.12 + 32.75 km from the hospital for their cancer treatment.
The most common types of cancers recorded were head and neck, such as cancers of the lip, tongue, buccal mucosa, soft palate, and gingivae (63, 42%), followed by cancers of the female reproductive system (44, 29.3%), and breast (24, 16%) [Table 1].
| Anatomical site of Cancer | Frequency (Percentage) |
|---|---|
| Head and neck | 63 (42%) |
| Female reproductive system (cervix, ovaries, endometrium) | 44 (29.3%) |
| Breast | 24 (16%) |
| Male reproductive/genitourinary system (penis, prostrate) | 4 (2.7%) |
| Stomach | 6 (4%) |
| Colorectal | 4 (2.7%) |
| Bone and cartilage | 5 (3.3%) |
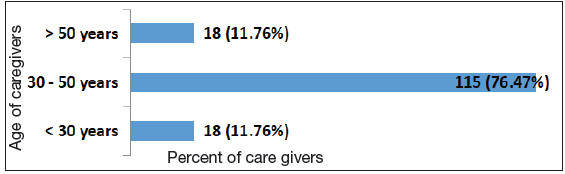
The mean age of the caregivers was 40.11 ± 11.03 years, and more than three-fourths (76.5%) of the caregivers were aged between 30 and 50 years [Figure 3].
- Distribution of caregivers based on their age (n = 150).
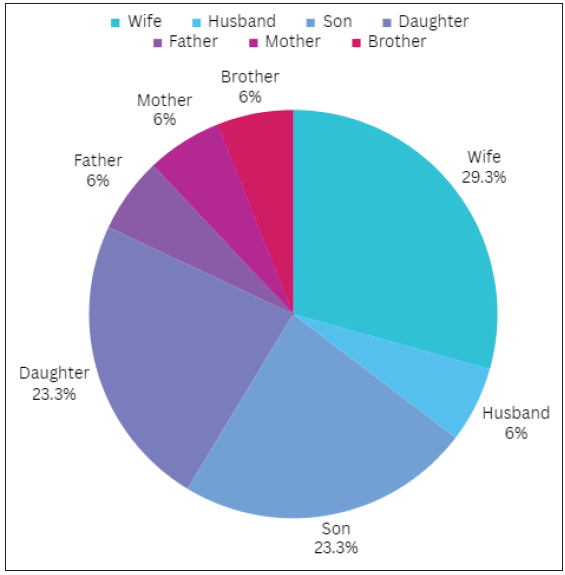
Nearly 47% of caregivers were children of the cancer patients (23.5% sons and 23.5% daughters), while 35.3% were spouses of the cancer patients (29.4% wives) [Figure 4].
- Distribution of caregivers based on their relationship to the cancer patients.
The majority of the caregivers were married (124, 82.3%) with one to two children (70, 47%), and 44 (29.4%) had no children. Most of the caregivers were literate, with 26 (17.6%) having completed high school, 44 (29.4%) educated up to graduation, 18 (11.7%) up to postgraduation, and 53 (35.3%) were illiterate. About 35 (23.5%) had professional occupations, 26 (17.6%) were skilled and semiskilled workers, and 53 (35.3%) were unemployed. It was also noted that 18 (11.7%) caregivers had comorbidities such as diabetes (11.7%) and hypertension (5.8%); addictions such as smoking and alcohol consumption were reported by nine (5.8%) caregivers.
The responses of the caregivers to the ZBI interview were analyzed [Table 2] and the total scores calculated for each caregiver were used to classify the caregivers based on the burden experienced by them [Table 3].
| Domain | Questions included | Mean Domain Score |
|---|---|---|
| Financial/physical strain | 10, 11, 12, 15, 17 | 3 ± 0.71 |
| Time/dependency strain | 1, 2, 4, 6 | 2 ± 1.15 |
| Emotional strain | 3, 9 | 3.5 ± 0.71 |
| Uncertainty | 7, 19 | 4 |
| Self-criticism | 21, 22 | 3.5 ± 0.71 |
| Total ZBI Score | Burden Category | Frequency | Percentage |
|---|---|---|---|
| 0 – 21 | Little or No Burden | 16 | 10.6% |
| 21 – 40 | Mild to Moderate burden | 24 | 16% |
| 41 – 60 | Moderate to Severe burden | 70 | 46.7% |
| 61 – 88 | Severe burden | 40 | 26.7% |
ZBI: Zarit burden interview score.
The burden scores on the “emotional strain” and “financial/physical strain” domains were found to be significantly higher among female caregivers. The caregiver role is often exclusively assumed by female caregivers, leading them to perceive the demands on their time from caregiving tasks as normal. Consequently, there is a lack of association of higher burden scores in the “time/dependence” domain for a female caregiver [Table 4].
| Domain | Mean Domain Scores | |
|---|---|---|
| Males | Females | |
| Financial/physical strain | 2.8 ± 0.56 | 3.4 ± 0.70 |
| Time/dependency strain | 2.1 ± 1.07 | 2.1 ± 1.12 |
| Emotional strain | 3.2 ± 0.92 | 3.8 ± 1.25 |
| Uncertainty | 3.8 ± 0.22 | 3.8 ± 0.34 |
| Self-criticism | 3.1 ± 0.64 | 2.9 ± 0.78 |
The caregivers with lower educational attainment showed higher burden scores in various domains. However, higher educational attainment was found to confer some degree of socioeconomic advantage and facilitated their exposure to wider social networks and resources that may mitigate the negative impacts of caregiving [Table 5].
| Domain | Mean Domain Scores | ||
|---|---|---|---|
| Illiterate | Upto Intermediate/Diploma | Graduation or Above | |
| Financial/physical strain | 4.2 ± 0.81 | 4 ± 0.64 | 3.4 ± 0.37 |
| Time/dependency strain | 3.5 ± 0.67 | 3.2 ± 0.82 | 3.1 ± 1.10 |
| Emotional strain | 3.1 ± 0.92 | 3.0 ± 0.92 | 3.0 ± 0.75 |
| Uncertainty | 3.5 ± 0.40 | 3.3 ± 0.47 | 2.9 ± 1.12 |
| Self-criticism | 2.9 ± 0.65 | 3.2 ± 0.58 | 3.4 ± 0.97 |
Caregivers with a shorter caregiver-patient contact time as a result of employment showed higher burden scores on the “self-criticism” domain and on the “self-criticism” and “time/dependence” domains. Meanwhile, unemployed caregivers reported higher levels of burden on the “financial/physical strain” domain [Table 6].
| Domain | Mean Domain Scores | |
|---|---|---|
| Unemployed | Employed | |
| Financial/physical strain | 4.2 ± 0.56 | 3.4 ± 0.37 |
| Time/dependency strain | 3.2 ± 1.07 | 3 ± 1.12 |
| Emotional strain | 3.1 ± 0.92 | 3.0 ± 0.75 |
| Uncertainty | 3.5 ± 0.40 | 3.5 ± 0.34 |
| Self-criticism | 2.4 ± 0.64 | 3.8 ± 0.57 |
Older caregivers and caregivers who were parents or spouses of the patients had higher burden scores on the “uncertainty” domain as compared to younger caregivers. Similarly, caregivers of patients with longer duration of illness also showed higher scores on the “uncertainty” domain.
DISCUSSION
In this study, 150 cancer patients were enrolled, each accompanied by one caregiver. The majority of the patients were males aged between 51 and 70 years, and most were married, with some being widowed or unmarried. A significant proportion of the patients were educated, although about a third were illiterate. Similarly, more than one-third of the patients were unemployed, while others were primarily unskilled or skilled workers. Head and neck cancers were identified as the most common type of cancer among the patients, followed by cancers of the female reproductive system and breasts.
The caregivers, predominantly aged between 30 and 50 years, were married with children. Nearly half of them were children, while one-third were spouses of cancer patients. The majority of the caregivers were literate and held professional occupations, while one-third were unemployed. Approximately one in ten caregivers had comorbidities such as diabetes and hypertension.
A similar study conducted in India by Ramasamy et al.,[1], which investigated the psychosocial challenges experienced by primary caregivers of patients with head and neck cancers in Tamil Nadu, utilized the ZBI. Their findings concluded that a majority (46.7%) of the caregivers reported experiencing mild to moderate burden, while 27% reported little to no burden. This contrasts with our study, where the majority of caregivers faced moderate to severe burden (46.7%), followed by severe burden (26.7%).
A study by Adeosun et al.[2] explored the correlates of caregiver burden among family members of patients with schizophrenia in Lagos, Nigeria, employing the ZBI and the Positive and Negative Syndrome Scale. Similar to our study, their assessment of burden scores revealed that female caregivers, older caregivers, caregivers with lower levels of education, and those who were parents or spouses of cancer patients experienced higher burden scores across various domains. Additionally, their study concluded that poor social support and lower educational levels of caregivers were predictive of higher burden scores in the “financial/physical strain,” “time/dependence,” and “emotional strain” domains. Furthermore, longer duration of illness, shorter patient-caregiver contact time, and being a female caregiver were predictive of higher burden scores in the “uncertainty,” “self-criticism,” and “emotional strain” domains, respectively.
On the same lines, the descriptive correlation study conducted by M. Vahidi et al.[3] among caregivers of patients with breast cancer in Iran, using the ZBI, found that activities of daily living, level of education, gender, and financial status were the determining factors of the burden of caregivers.
There are a few limitations to our study. Being a cross-sectional study, the experiences of the caregivers throughout the illness trajectory of the patient could not be obtained. However, further research with a longitudinal study will improve our knowledge of caregiver experiences throughout the illness trajectory. Knowledge gained from the study can also be used for intervention such as respite care and social and financial help to caregivers to improve their coping and decrease their burden. With our study, we suggest that cancer needs a holistic approach. Not only the cancer patients but their caregivers need intervention such as psychological, social, and financial help to improve their coping and decrease their burden.
CONCLUSION
Caregiving impacts the physical, emotional, financial, and social aspects of a caregiver’s life. Caregivers adopt active coping strategies to overcome the impacts of caregiving. The majority of the caregivers experienced moderate to severe burden, while most scored low on quality of life. Findings from this study point to high proportions of elevated psychological distress among family caregivers of cancer patients. Multidisciplinary arrangements are necessary to meet caregivers’ needs.
Author contribution
Subbiah Shanmugam responsible for Guide and proof reading. Arun Victor Jebasingh preparation of proof reading and draft creation. Suyash Singodiya preparation of research topic selection, data collection, review of literature, drafting of article, statistics and results and initial draft creation.
Ethical approval
The research/study approved by the Institutional Review Board at Government Kilpauk Medical College, number 1106/2023, dated 10th January 2023.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of AI-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Psychosocial issues among primary caregivers of patients with advanced head and neck cancer – a mixed-method study. Indian J Palliat Care. 2021;27:503-12.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Correlates of caregiver burden among family members of patients with Schizophrenia in Lagos, Nigeria. Schizophr Res Treatment. 2013;2013:353809.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Other side of breast cancer: Factors associated with caregiver burden. Asian Nurs Res (Korean Soc Nurs Sci). 2016;10:201-6.
- [CrossRef] [PubMed] [Google Scholar]




